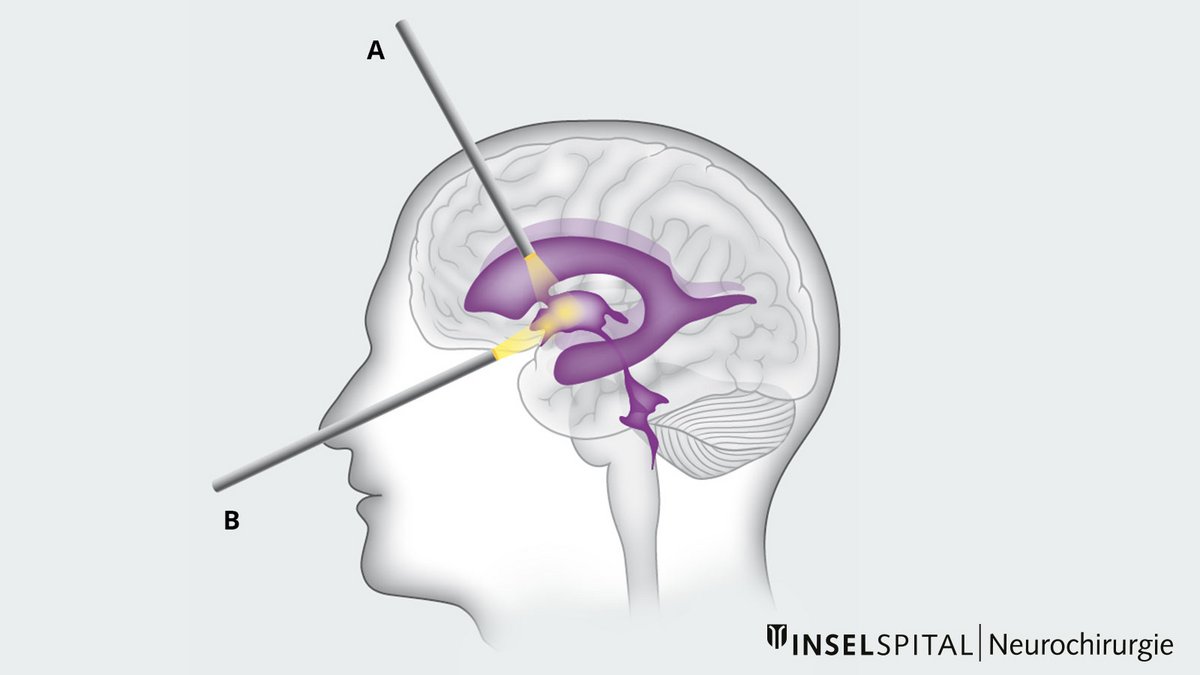
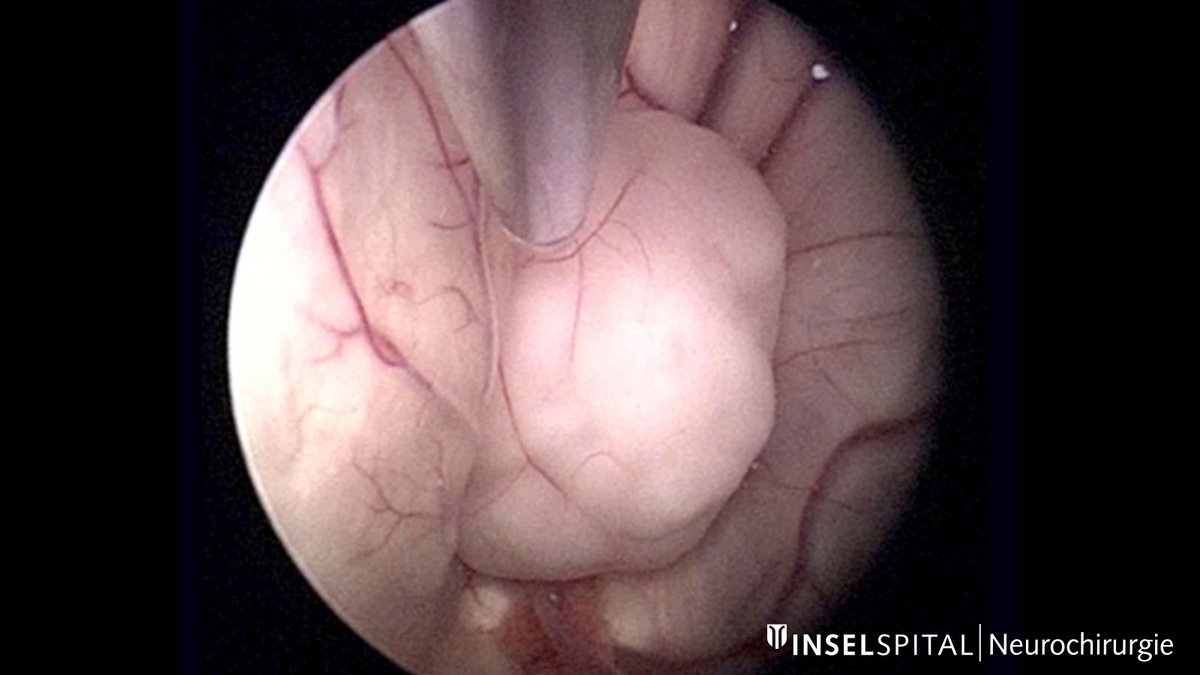
Neuroendoscopy is an important procedure in neurosurgery and is used regularly. It involves the use of special endoscopes equipped with a camera and light source. These enable high-resolution images to be obtained from deep within the brain, such as the brain ventricles or cysts, through very small incisions. At the same time, microinstruments can be inserted via the endoscope, allowing procedures to be performed with minimal invasiveness and under direct visualization.
How are endoscopes used in neurosurgery?
Endoscopy has undergone significant technological advances in recent decades and is now indispensable in everyday neurosurgical practice *.
Endoscopes are used to
- support microsurgical operations, for example to provide a better view of areas that are difficult to see, or to
- perform procedures entirely neuroendoscopically – for example in the area of the cerebral ventricles.
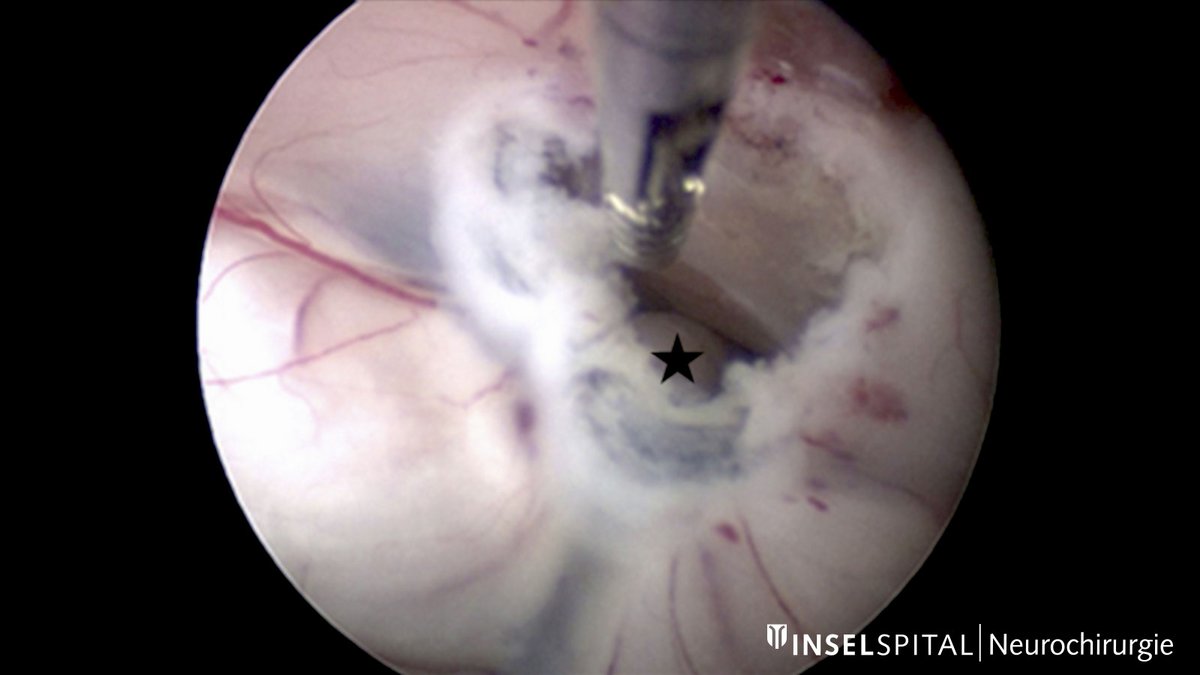
Surgeons have a variety of tools at their disposal, including endoscopically usable lasers, bipolar electrodes, and grasping forceps *.
If necessary, endoscopes can be used in combination with a neuronavigation system to ensure additional orientation safety in addition to visual control.
Which operations are suitable for endoscopic procedures?
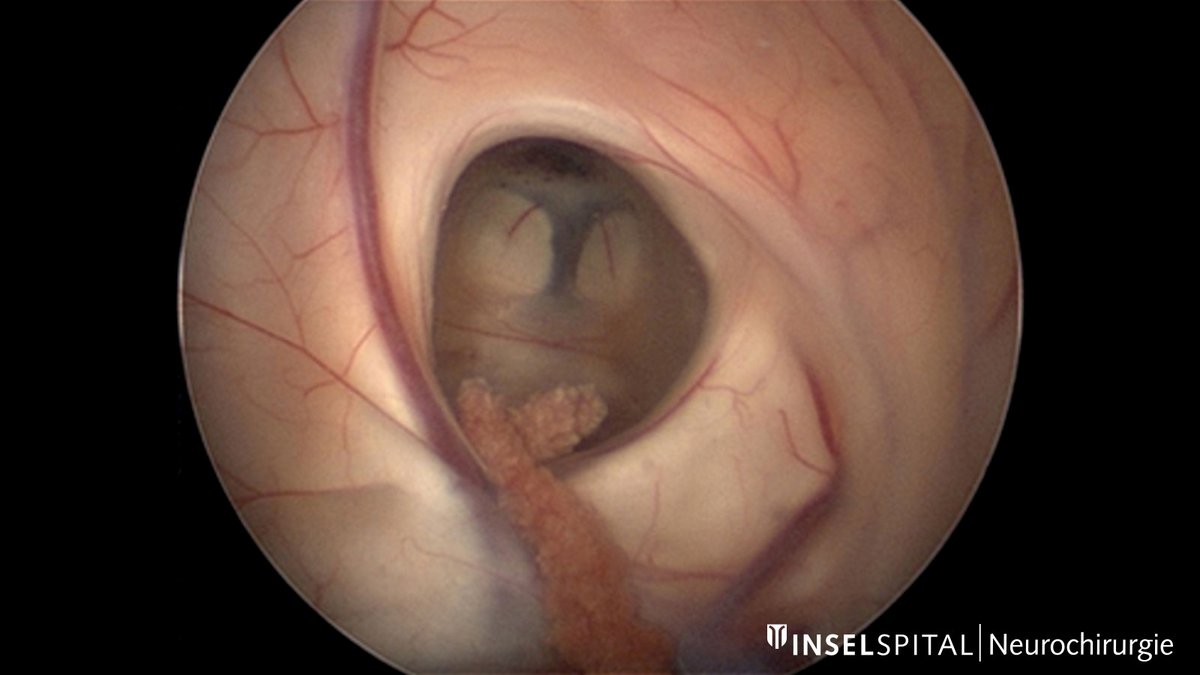
Neuroendoscopic surgery is primarily performed in the area of the cerebral ventricles and at the base of the skull. Tumors in the cerebral ventricles can obstruct the flow of cerebrospinal fluid (CSF), leading to enlargement of the ventricles. This creates a more accessible surgical field for the surgeon *. The lateral ventricles and the third ventricle are particularly suitable for endoscopic procedures.
Hydrocephalus occlusus
Hydrocephalus is usually treated with a shunt that drains cerebrospinal fluid (CSF). In hydrocephalus occlusus, also known as occlusive or obstructive hydrocephalus, the drainage of cerebrospinal fluid is impeded by a blockage or narrowing of the ventricles or the cerebrospinal fluid pathways. In this case, endoscopic surgery can help restore the natural flow of cerebrospinal fluid and thus avoid the need for a shunt. In a procedure known as endoscopic third ventriculocystostomy (ETV), the floor of the third ventricle is opened so that cerebrospinal fluid can flow out again.
It is rare for only the temporal horns of the cerebral ventricles to be congested, which may occur, for example, secondarily as a complication after tumor surgery. In some cases, endoscopic surgery may also be a treatment option *.
Arachnoid cysts
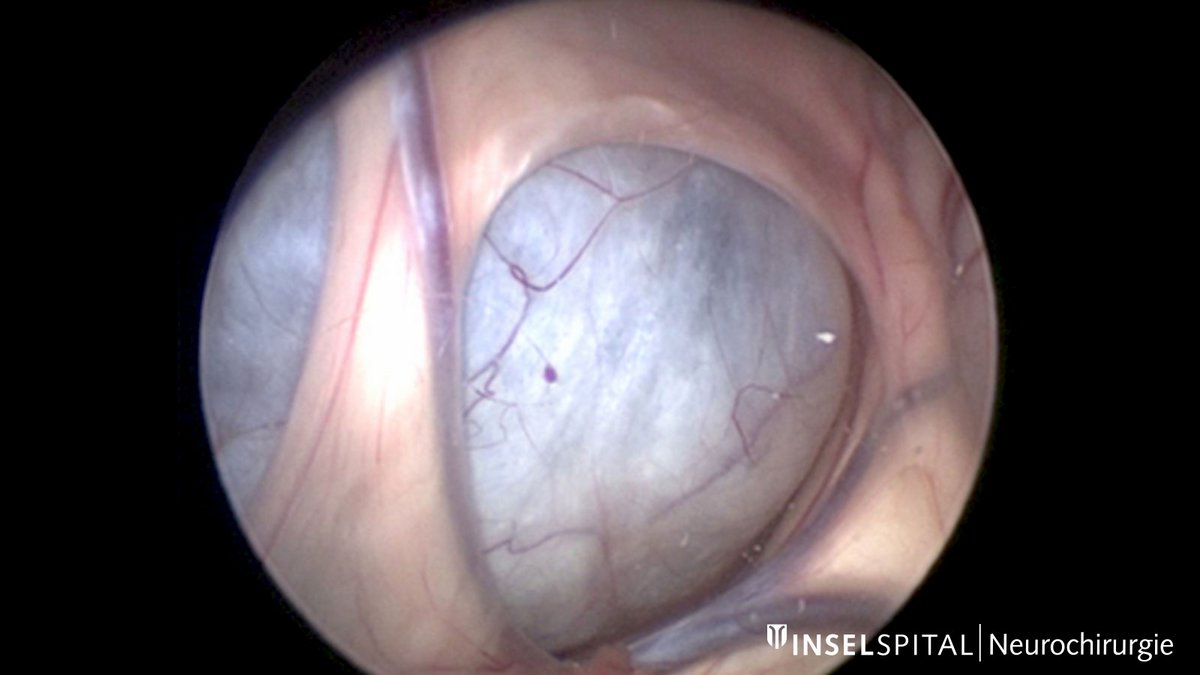
Arachnoid cysts are benign cystic changes of the middle meninges arachnoid, which are primarily asymptomatic and rarely require surgical treatment.
However, if cysts cause symptoms or grow larger, a procedure known as cyst fenestration may be necessary. This involves opening the cyst so that the fluid can drain out. Depending on the location and findings, this procedure can be performed using a minimally invasive, purely endoscopic approach.
Suprasellar arachnoid cysts are particularly suitable for this procedure if they lead to a hydrocephalus. The dilated ventricles allow good access and the possibility of large fenestration of the cyst, which significantly reduces the risk of recurrence. Study data show that repeated fenestration of suprasellar cysts is necessary only in the rarest of cases *.
However, the neuroendoscopic surgical procedure is not limited to suprasellar arachnoid cysts but can also be used for cysts in the middle and posterior fossa if sufficient access is available *.
Colloid cysts
Colloid cysts are benign cavities lined with a thin layer of cells and filled with a viscous substance. They are often located in the third ventricle and, depending on their size and location, can block the flow of cerebrospinal fluid.
Very small, asymptomatic colloid cysts usually do not require surgical intervention. However, if the colloid cyst causes symptoms or if the cyst has reached a certain size, surgical removal is generally recommended *.
If surgical cyst resection is necessary, it can be performed either microsurgically or, in favorable cases, purely endoscopically, depending on the location and size of the cyst.
Tumors
Endoscopic biopsy
Brain tumors are usually operated on microsurgically. An exception are intraventricular or paraventricular tumors, i.e., tumors that grow in the brain ventricles or in close proximity to them. These do not always need to be surgically removed; some of these tumor types respond well to other forms of treatment.
However, a fine tissue examination (biopsy) is almost always necessary for diagnosis and planning further treatment. If the tumor is located in an easily accessible area,an endoscopic biopsy is possible. This gives the surgeon the advantage of being able to select the biopsy site precisely thanks to a direct view of the tumor. This increases the accuracy of the examination and also makes it possible to stop minor bleeding immediately.
Since tumors in the brain ventricles can impede the flow of cerebrospinal fluid, a decompression procedure such as an endoscopic third ventriculocisternostomy or septostomy can be performed at the same time as an endoscopic biopsy, if necessary.
Fully endoscopic tumor resection
In some instances, a fully endoscopic removal of an intraventricular tumor is possible. Tumors with a moderate blood vessel supply, a soft consistency, and a size of < 2–3 cm are particularly suitable for this *.
However, if the tumor shows adhesions to structures such as the fornix or the thalamostriate vein, a complete resection is often not possible in order to avoid injury to these structures *.
The disadvantage of neuroendoscopic tumor surgery for the surgeon primarily lies in the restricted maneuverability afforded by the endoscope and the absence of bimanual dexterity, as is possible in an open surgery.
Pituitary and skull base surgery
Endoscopes provide surgeons with excellent visibility and illumination of the surgical site, even through narrow access routes. Angled optics also allow areas to be viewed that would not be visible with a surgical microscope.
In addition to the classic access routes through the skull, minimally invasive surgery via the nose (transnasal) is also possible. In this way, for example, pituitary tumors can be completely removed under direct visual control.
Surgery in the area of the brainstem and cranial nerves
Many sensitive structures lie very close together in the brainstem and around the cranial nerves. Using an endoscope makes it possible to look «behind» these structures without damaging them. This helps the surgeon assess the individual anatomy and identify causes of disease—for example, a vascular loop pressing on a nerve that can trigger trigeminal neuralgia or hemifacial spasm.
Neuroendoscopy allows such vascular-nerve conflicts to be precisely visualized and surgical treatment to be monitored directly under visual control. Endoscopic visualization offers the particular advantage of being able to view structures from different angles, especially in the cerebellopontine *.
Neuroendoscopy at Inselspital
Generally, we plan surgeries and the use of various surgical techniques individually for each patient. The appropriate surgical procedure will be precisely explained during the consultation in our clinic and during the pre-operative informed consent discussion.
For the listed medical conditions, either a purely neuroendoscopic or a neuroendoscopically-assisted operation may be appropriate.
-
The Principles of Neurological Surgery. Archives of Neurology And Psychiatry. 1942;48(1):162.
-
Gaab M, Schroeder H. Neuroendoskopie und endoskopische Neurochirurgie. Der Nervenarzt. 1997;68(6):459-465.
-
Cappabianca P, Cinalli G, Gangemi M, et al. Application of neuroendoscopy to intraventricular lesions. Neurosurgery. 2008 Feb;62 Suppl 2:575-97; discussion 597-8.
-
Krähenbühl A, Baldauf J, Gaab M, Schroeder H. Endoscopic temporal ventriculocisternostomy: an option for the treatment of trapped temporal horns. Journal of Neurosurgery: Pediatrics. 2013;11(5):568-574.
-
Caemaert J, Abdullah J, Calliauw L, Carton D, Dhooge C, van Coster R. Endoscopic treatment of suprasellar arachnoid cysts. Acta Neurochir (Wien). 1992;119(1-4):68-73.
-
Schroeder H, Gaab M, Niendorf W. Neuroendoscopic approach to arachnoid cysts. Journal of Neurosurgery. 1996;85(2):293-299.
-
Mathiesen, T., Grane, P., Lindgren, L. and Lindquist, C., 1997. Third ventricle colloid cysts: a consecutive 12-year series. Journal of Neurosurgery, 86(1), pp.5-12.
-
Gaab M, Schroeder H. Neuroendoscopic approach to intraventricular lesions. Journal of Neurosurgery. 1998;88(3):496-505.
-
D'Angelo V, Galarza M, Catapano D, Monte V, Bisceglia M, Carosi I. Lateral Ventricle Tumors: Surgical Strategies According to Tumor Origin and Development – A Series of 72 Cases. Operative Neurosurgery. 2005;56(suppl_1):ONS-36-ONS-45.
-
Teo C, Nakaji P, Mobbs R. Endoscope-Assisted Microvascular Decompression for Trigeminal Neuralgia:Technical Case Report. Operative Neurosurgery. 2006;59(suppl_4):ONS-E489-ONS-E490.